


Tough Calls: Case 5
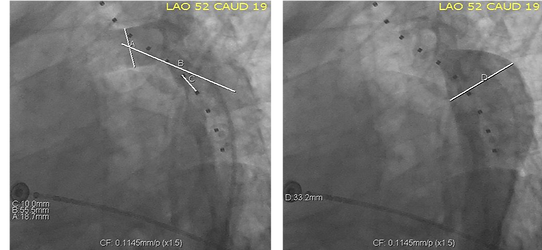
Severe Coarctation Immediately Distal to Left Subclavian
Imagine how you would work through each case. What equipment would you select and what would you do first? After having a go at it, see what our panel would do in the same situation. This exercise highlights the many possible approaches to a difficult problem. By seeing what others would do after thinking it through yourself, you will gain an understanding of the spectrum of approaches to a problem.
32 year old male nurse; difficult to control hypertension, exercise leg discomfort

Expert Approaches
Hover over an experts image to view their approach.

This case, I would place a bare metal stent 18mm diameter x34-43 mm long (CP or AndraStent). Place on BiB balloon during RV pacing for accurate positioning.
Dr. Ziyad Hijazi
Professor of Pediatrics & Medicine, Weill Cornell Medicine
Chair, Department of Pediatrics and Director, Sidra Cardiac Program

•Concern that CoA very short in close proximity to the LSCA
•Consideration for open cell stent on 20mm balloon, but will need to consider covered stent if severe stenosis or dissection/tear/pseudoaneurysm forms with intervention
•Recommend access in left radial artery for imaging/monitoring
•If covered stent required, can position the CP covered stent from distal transverse arch through the CoA and jail/seal off the LSCA and then perforate through the covered stent from the left radial access, balloon the cells of the covered stent and consider stenting through the covered stent to maintain LSCA patency
Dr. Matthew Crystal
MD, FACC, FSCAI
New York-Presbyterian & Morgan Stanley Children's Hospital
Assistant Professor of Pediatrics, Columbia University Medical Centre

-
Aim to treat with a bare stent, jailing LSCA (sized to arch diameter 19mm)
-
Access : 6f RRA to image from above (pigtail), 8f RFA sheath + proglide (then upsize to 12F)
-
Cross from below using Amplatzer extrastiff wire
-
Long 12F sheath to arch and deploy CP bare stent mounted on 18 or 20mm BiB balloon - extend from mid arch to just beyond coarctation; likely ~ 40mm.
-
45mm CP stent will shorten to 37mm on 18mm balloon, thus custom made 50 or 55mm stent may be required.
-
Post dilate as necessary, aiming for good apposition at arch
-
I would leave LSCA jailed by stent
Dr. William Wilson
MBBS, PhD, FACC
Consultant Cardiologist at Royal Melbourne Hospital

•Double balloon COA stenting with Covered stent
•One wire in LSCA and one in AAO
•Minimum balloon Diameter 10 mm. May use 12 mm
Dr. Zahid Amin
MD, FSCAI, FAHA, FAAP
William B. Strong Chair & Professor & Section Chief Division of Pediatric Cardiology
Children's Hospital of Georgia, Augusta University

•Vascular surgery for carotid-subclavian bypass; move to cath lab under same anesthesia
•Femoral artery access only
•10 zig, 60 mm CP covered stent on 20 mm BiB, place to full diameter, with the top of the stent at line “A”
MD, FSCAI
Dr. Nathan Taggart
Pediatric Interventional Cardiologist
Assistant Professor of Pediatrics
Mayo Clinic

-
Juxtaductal coarctation with proximal descending aortic aneurysm
-
Right femoral access, pigtail angiography
-
Balloon with 18mm balloon
-
Stent (Max LD), jailing left subclavian artery, up to 18mm
-
Surveillance of prox descending aortic aneurysm. If there is pseudoaneurysm or growth, would need to place TEVAR graft extending from aortic arch to descending aorta. In this case would likely need to occlude left subclavian artery to prevent Type 2 endoleak. Left carotid subclavian bypass after subclavian occlusion as elective procedure if clinically indicated.